Centers for Disease Control, in the U.S.A. record roughly about 300K concussions per year. These are just from sport, not to mention the concussions sustained during other types of accidents, nor does this number reflect those concussions that are considered “Sub-concussive Brain Trauma” (SCBT) or Chronic Traumatic Encephalopathy (CTE).
It appears that high-school football players sustain far more concussions and more often than those athletes at the collegiate and professional level. Concussions in female athletes are on the rise as well.
In a single 80-yard drive, a NFL lineman, can sustain up to 18 SCBT’s. Over a 10 year career, they would have sustained roughly 15,000 SCBT’s! This is according to Dr. Robert Cantu, a prominent neurosurgeon from Boston MA.
SCBT is a cumulative ticking time bomb, waiting to explode. Becoming more apparent as the athlete ages, resulting in symptoms like dementia known as chronic traumatic encephalopathy (CTE), a progressive, degenerative brain disease, just to name few. This is similar to what boxer’s experience. It is known as “dementia pugilistica.” SCBT injuries are especially traumatic; due to the fact the athlete may not show any overt symptoms of a concussion, despite having received multiple blow the cranium. It is only till later in life that the athlete may show signs of Traumatic Brain Injury (TBI).
SCBT can be represented as bruising to the brain, or micro-trauma, which cannot be seen, much like if one where to sustain such an insult to the thigh, for example. These micro impacts can easily diminish the threshold of partial and/or permanent brain trauma.
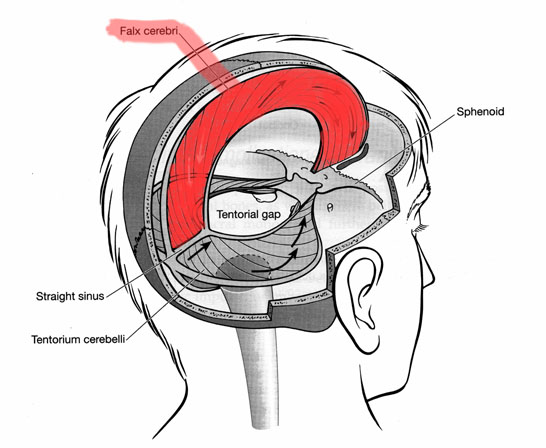
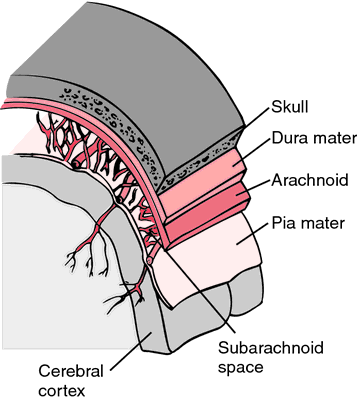
TBI’s involve a sudden yet violent anterior-posterior, acceleration and de-acceleration of the brain, that may or may not be accompanied with a large amplitude rotational forces as well. It is this sudden acceleration and de-acceleration that force the brain to violently move inside the skull, only to have to come to a dead stop, and re-coil back the opposite way it came from. This action can distort the cranial membranes (i.e. falx cereberi and the tentorium cerebelli). It is this disruption, amongst other structures, that is usually compromised. The alteration of these two membranes can alter fluid dynamics of cerebral spinal fluid, as it flows throughout the cranial cavity. The disruption of these membranes can also affect brain function.
At the cellular level, according to Dr. Allen Hovda, Director of the Brain Injury Research Center at UCLA, the nerve cells become stretched or twisted, releasing potassium into the extracellular matrix, which in turn, depolarizes the cell allowing calcium to reduce cellular function. The resulting consequence is an increase in amnesia, confusion and a loss of consciousness, via the inhibition of cellular function of the impacted cells and the subsequent surrounding tissue. The inhibition of cellular function causes the brain to increase its uptake of blood glucose, which can result in a overproduction of lactic acid. The lactic acid, itself, begins to inhibit brain function. Blood flow diminishes by roughly 50%, to prevent swelling. It will take roughly 10 days before normal blood flow to the brain is restored, depending upon the extent of the damage to the surround tissue. It is during this time period, which if the athlete sustains another SCBT, which in turn, will not only delay the healing process, but also will never allow the brain tissue to completely heal itself.
…Personally, he is extremely caring and passionate about any fellow human being and professionally, an endless researcher of new methods and understanding of how the mind and body works making him in my opinion second to none, of all the people on his field of expertise that I had the opportunity to meet and deal with throughout the World, in terms of training, recovery & regeneration and physiotherapy. Yusef’s approach to treat the root of the problem in detail, instead of the symptoms, sets him far apart from most of the conventional practitioners. I’ve witnessed many times while working abroad with Yusuf, how much his professional peers from different countries such as Italy, Germany and Spain had praise and the highest regards for his talent and knowledge… Continue Reading “Armando Costa”
…Yusuf is an excellent speed & strength conditioning, & regeneration specialist…I have personally worked with him for over 13 years now, & referred him to various consulting contracts in various sports, ranging from cycling, hockey, swimming & many others… he has an excellent grasp of Regeneration and Periodization… Due to his understanding of such concepts, I have on several occasions, have asked him to lecture for me in my absence. I would highly recommend him for work with in planning, regeneration & conditioning for high-performance athletes. Continue Reading “Dr. Tudor O. Bompa, Ph.D.”
World Renowned Planning Specialist & “Father” of Western Periodization Professor at York University, Toronto, Specializing in Elite Coaching Methodology
A genius when it comes to providing real measurable results by building a strong base and fixing weak areas first. Yusuf provided some great holistic plans for nutrition that made a huge difference in my health, I used to get the cold/flu very often but that’s all gone now! … Continue Reading “Muneeb Cheema”
…The symptoms from Concussion Syndrome have reduced a lot, which in turn has allowed me to train again at a level required for me to achieve my personal goals. The fundamentals taught to me by Yusuf have made me understand the necessary steps and precautions to be taken in order to decrease my injury potential. I am much stronger, my range of motion has improved, and I’m able to train without fear of residual issues arising after an intense training session. It’s one thing to perform at a high level but another to actually perform these athletic abilities consistently without fear of injury or reprisal. Continue Reading “Troy Dos Santos”
100 meters in 10.26, Former Canadian National Team Member & Elite Performance Enhancement Specialist
…His anatomical knowledge and progressive/holistic approach have been instrumental in allowing me not only to recover from injury-but to really reconstitute how my body responds to training. He’s helped to regain and rebuild a solid foundation of strength and flexibility while helping me understand the intricacies and nuances of training… Continue Reading “Steve Ballstadt”
Principle Percussionist “Blueman Group” Live Theater Production Boston, M.A., U.S.A.
…His views on training and recovery are unparalleled and I started producing results very quickly winning races in my age category…I had a concussion and an injured
shoulder/rotator cuff. Most likely a nerve impingement. I didn’t even bother going to the doctor. I walked into his office a mess, but walked out 3hrs later ‘floating’. I had regained full mobility in my shoulder and drastically minimized the ‘fogginess’ associated with concussions. I was in awe!
In 2000, I severely sprained my left ankle. Torn ligaments, swollen, black and blue. With his treatment protocols, I was walking within 3 days and had fully recovered and resumed training within 3 weeks. This would normally be a one-two month process anywhere else. 3 weeks! Very impressive! These are just a few notable stories of many that I have.
I would highly recommend his services if you are looking to:
• Achieve peak physical fitness for competition in any sport
• Recover from long standing injuries that has EVERYONE else baffled.
…Physiotherapists were working treating local issues in my body, while Yusuf was able to pin point the actual cause of the issue and help alleviate it. He has a wealth of knowledge and parts of the work he does is almost magical. I still can’t believe how simple he makes things… Continue Reading “Paul Rabindran”
…I have dropped three seconds in the 400m and I plan to drop another three seconds in a few months. Overtime after working with the system I’ve noticed that my spring after my foot touches the ground is becoming more powerful so I’m spending less time on the ground which means that most the time I am in the air which equals to faster times and less work and stress loads on my body. I have also noticed a reduction of restrictive movements as well as a lesser risk of injury potential which is a big thing for me since I had big problems with my hamstrings in the past and now that I’ve learned to listen to my body and react to what it’s telling me my injury potential has reduced exponentially. Continue Reading “Marcus Collins”
…He has an amazing knowledge of human body and function from a multi-disciplinary approach. I was back to playing squash within a few months and avoided unneeded surgery for a slight meniscus tear. If you are looking for a quick fix, you are in the wrong place. If you are looking for sustained results, and are prepared to do your homework, Yusuf is great. Continue Reading “Phil Mercurio”
…Working with Yusuf, my times have dropped from 10.56 sec to 10.10 in less than 4 weeks, with proper nutrition, regeneration and speed training. He is very capable and knowledgeable specialists in the field of long-term planning, regeneration, strength, speed training. Continue Reading “Antonio Williams”
… I definitely noticed a reduction is restrictive movement and as a result my injury potential was significantly reduced…Since I started with Yusuf my injury potential has completely minimized, my strength, conditioning, power, speed, endurance and flexibility have increased exponentially and as a result my performances have improved significantly. Continue Reading “Colin Ramasra”
Professional Squash Player ranked #233 in the world, #1 in Trinidad & Tobago
The work done here on treating concussions and injuries transcends anything I have seen in the mainstream regiment. Yusuf has a profound understanding of what it means to be a “healer”… Continue Reading “Paul Burke”
…he has specific sport over sight that he can administer into the rehab and re-conditioning training. He also has vast level of knowledge that has helped me become more aware of how to train more effectively helping improve my overall performance.
It took me about 4 weeks of the training before a saw the results. The execution of my runs became more efficient Any person looking to improve their performance will benefit from working with Yusuf. His Knowledge and ability to break athletes down is a gift that you can’t learn. Any athlete working with Yusuf will be at an advantage over there competitors (i.e. service, obtained better performance, professionalism, higher standard of business practice, able to deliver performance in a very short period of time with “outside the box” conditioning & regenerative methods) Continue Reading “Mike Whitely”
Yusuf has a unique understanding that we weren’t able to find in any therapist or doctor. Also, Yusuf works on fixing problems not just a “band-aid” approach.”
800m Runner, University of Southern California NCAA Division 1
…Yusuf has been able to address the root cause of my recurring sport injuries in order to allow me to train better and more effectively in less time that I thought possible. Continue Reading “Matt Loparco”
…suffers from osteoarthritis of the hip…as a result has become quite immobile and the surrounding muscles have become quite weak. After 2 years of training with Yusuf, I am now able to perform exercises that are unheard of form people in my condition… Continue Reading “Michael Zimmerman”
Former Director of Tennis Mayfair Racquet & Fitness Clubs
…he was among the most honest and exceptional and creative forces in the sports training and planning industry. He introduced me to several techniques that radically changed my perspective on training and diet methods for elite athletes. Continue Reading “Dr. Michael Hollis B.Sc., N.D.”
Naturopathic Doctor at Link Medical Center, San Francisco
Yusuf is extremely knowledgeable in the areas of Elite Level Planning, Speed & Power Development, as well as Strength Training for Speed-Power sports. I have worked with Yusuf in the development of videos regarding “off-ice conditioning for hockey players” and have asked him to guest lecture on occasion at York University… Continue Reading “Dr. Dave Chambers, Ph.D.”
Professor at York University, Toronto, Specializing in Elite Coaching Methodology, Former Assistant Coach to the Quebec Nordiques (Now the Colorado Avalanche N.H.L. team)
Mr. Omar was extremely thorough in implementing a program complete with a comprehensive initial assessment; dietary recommendations; seminar and workouts. He focused his approach to address the specialized needs of our team and our goal of interest increasing overall athleticism…Mr. Omar took every opportunity to educate us on the theories of conditioning, met with parents, kept a vigilant eye for a player’s performance and provided us with a unique format of reporting. To date, the girl’s overall conditioning has increased over 20%. Continue Reading “Tony D’Amato”
Licensed FIFA Coach & Head Coach Etobicoke Energy Soccer Club OYSL Girls U14
There is no doubt Yusuf has a gift. He worked with my son after he sustained a concussion in a hockey game. He brought my son to a state of normality, which we thought he would never get back. He genuinely cares about his patient’s well-being and consistently asked about his progress. I recommend him to everyone I speak with… Continue Reading “Marisa Duarte”
…He had suffered a reoccurring ankle problem, which had been going on for about 6 months. Prior to this he had been to a physiotherapist, a chiropractor and a sports medicine doctor. Their diagnosis altered from a chronic sprained ankle to a broken bone in his foot. One of the specialists stated it would be unlikely he would ever be able to run competitively again which caused major frustration for Ben…
Yusuf took the time to understand the real nature of Ben’s injury and worked extensively with him to ensure the injury was treated appropriately. Yusuf explained how Ben’s alignment had been affected and through intensive therapy and support Ben was able to recover 100% from his injury and began to perform and train better than ever. As a result, Ben has had a very successful running career to date and is now headed to University of Toronto and will be a member of the elite U of T track team.
We owe so much to Yusuf, for his time, his patience and his expertise. I truly believe without his amazing insight into Ben’s injuries and his understanding of the human body, Ben would not be training and running competitively today. We have recommended Yusuf to many athletes Ben has trained with and the results have always been beyond expectation. Both Ben and I highly recommend Yusuf and believe he has made a lasting impact on Ben’s athletic abilities. Continue Reading “Laurie Campbell”
Full Testimonial: I have been working with The System for approximately 4 months. A friend recommended me to The System and at first I was skeptical but after speaking with Yusuf I realized that everything he does aims to better me as an athlete as well as a better person. And even after a few weeks I… Continue Reading “Marcus Jabari”
…Not only could Yusuf help with the healing, but he could also be my trainer to keep me strong, while recovering, and not over-work my injuries. Continue Reading “Ally Christiani”
200m / 400m Runner, Illinois State University (ISU), NCAA Division 1
Yusuf worked with our national swimmers in the area of strength, flexibility and power training…the learning curve that our staff went through as well as the improvements by our national swimmers was tremendous… Continue Reading “Chuck Meklensek”
…the best methods & techniques come from the trainers who think ‘outside-the-box’. These trainers are the true pioneers, pushing the boundaries of human limits. Yusuf Omar is one of these select few individuals. I have personally experienced & observed the results of his methods, methods that are light years ahead of what is currently considered ground-breaking. Continue Reading “Dr. Nikos Apostolopoulos Ph.D.”
Recovery & Regeneration Specialist, Founder of “Stretch Therapy” & “Microstretching”